Since COVID usually kills via pneumonia, and insufficient vitamin D appears to be a surprisingly large risk factor in respiratory infection, it’s probably pretty important to keep vitamin D levels sufficient (which in most people means supplementing it specifically, esp if there’s any quarantine that affects food).
Studies:
Note: In the summary post, this comment thread suggests getting only normal amounts of vitamin D.
From Lifestyle interventions to increase longevity:
There’s also the bad news that multivitamins mostly don’t do anything. There has not been found an alternative to eating a variety of nutrient-dense whole foods. Though vitamin D supplementation appears to be quite beneficial.
(FWIW, I just purchased from the Amazon link!)
Scott Alexander says Vitamin D is (TL;DR) just good for bone health, even though studies exist saying otherwise.
https://slatestarcodex.com/2014/01/25/beware-mass-produced-medical-recommendations/
wdyt?
Incentive sperometers are often used for the prevention of pneumonia. Maybe this suggests using those as well?
What would be the appropriate dose of Vitamin D?
The large effects on children is an odd example (poor example?) to point at since children have been reported to have the least harm from COVID-19.
Is there any reason to worry copper tape might be less effective than the copper used in experiments? (I haven't read methods to see if they describe the source of the copper) For example, a lot of copper is designed to be resistant to oxidation - does that matter?
You can get vitamin D from sunlight exposure. For white people, this doesn't take long, probably minutes (around noon) of direct exposure on your face and arms. If your skin is darker, it takes longer. You have to expose more skin for longer periods. Black people maybe can't get enough at high latitude and will have to take the pills. If you're supplementing this way, you do have to actually step outside for a bit. Exposure through windows that block UV is not going to work. Obviously, sunscreen will prevent some exposure.
If you get a sunburn, you waited t
...Advice: Use gloves or wash your hands after handling delivery packages, and be careful not to touch your face while handling them.
Model:
In photos of Amazon fulfillment centers, the workers appear to mostly be wearing fabric work gloves, not disposable gloves. Workers touch both the outer cardboard box and the item; but if the item has its own packaging, anything inside of that will probably have been untouched since manufacture, which is probably long enough.
I also spray all deliveries with disinfectant and put them for a waiting room for days. Also disinfect floor where they were and the bottoms of my shoes.
Do you mind elaborating on how you reconcile your model with the 1st CDC link you list in your research? "In general, because of poor survivability of these coronaviruses on surfaces, there is likely very low risk of spread from products or packaging that are shipped over a period of days or weeks at ambient temperatures" And my interpretation of the 2nd JHI link is that since cardboard is perhaps closest to wood/paper, then the persistence is about 1-4 days, which seems to indicate a relatively low risk (at least compared to other surfaces). I think taking your advice is reasonable because it only increases safety; I just wanted to better understand what we think the risk level is.
How about using UV lamps and ozone in bathroom to sanitize the deliveries? This might be particularly useful for groceries.
Unexpected difficulty: if I open packages with scissors wearing gloves, I tend to cut my gloves. Maybe this would work better now that I have a box cutter?
Use hand sanitizer or wash hands with soapy water frequently- after touching any doorknob exposed to an epidemic, at a minimum. (This includes doorknobs that only you touch, if there's a chance that you're in an infections asymptomatic state). Other triggers include the normal cases of before cooking and before eating.
Tl;dr Putting copper tape on commonly-touched surfaces is a high-value thing to do in the case you’re actively trying to avoid infection, since copper kills viruses and ~~50% of viral disease is from hand-to-surface-to-face contact (h/t Adam Scholl for hypothesis) [ETA: coronavirus seems to have mostly (?) respiratory droplet transmission, so this prior is less relevant but still worth intervening upon]
Amazon link (sadly, probably one Amazon item that won’t go out of stock)
Metals killing bacteria is well-documented, like all the very consistent results in this paper comparing 9 metals (lead kills slightly better than copper but that unfortunately extends to the humans; zinc and some other metals also kill pretty well, only two did not). Within an hour, copper dropped CFU from 10^6->10^1 (the measurement threshold). Zinc took 2 hours, nickel 4.
Unfortunately, this isn’t in widespread use in hospitals yet. But when it does, copper on the most-touched surfaces of an ICU appears to reduce infections by about half (bed handles, chair armrests, nurse call buttons, and a few others). But these are in very high-germ-load environments. What happens in a normal home?
First, how much of disease spread is from hand-to-surface vs airborne or hand-to-hand? I lost the citation and it wasn't well backed, but apparently you don't catch colds through suspended particles very often (someone has to sneeze within 6 feet or exhale in your face lots). And hand-to-hand contact spreads it more efficiently but (one paper said) less frequently than hand-to-surface-to-hand, especially in environments without lots of high-fiving and hand-shakes. Plus, the study saying 50% infection reduction from copperizing main surfaces would fit well with a base rate of ~70% hand-to-surface infections and, of these, ~70% of touches in the ICU got sanitized by the dangerous surface metal coverings. But 70% sounds like a lot so I’m going to be a little conservative and just say 50%.
Now, it’s hard to figure out how many things you’d need to cover with copper to reduce most of this. But some typical commonly-touched shared items are:
Depending on how many people you are sharing touch-space and not air-space with, I expect covering these in copper could reduce infection by anything from 1 to 50%, though I expect in a typical house of four people who sometimes venture outside and don’t know about never touching your face, you’d get an effect roughly between 15 and 40%.
[UPDATED, thanks to various people who caught errors in V1 and pointed out V2] New NIH study of COVID half-life in aerosol or on surfaces V1 with errors: https://medrxiv.org/content/10.1101/2020.03.09.20033217v1 , V2 hopefully error free: https://www.medrxiv.org/content/10.1101/2020.03.09.20033217v2.full.pdf (H/T @AndyBioTech)
2.4-5.11 hours on copper, in contrast to 10.5-16.1 on steel or 13-19.2 on plastic
This study describes "detecting viable virus" as having a threshold of 10^0.5 TCID50/mL, and they assume exponential decay of viable virus particles.
I'm really confused by their numbers, tho; it looks like cardboard has a hundred-fold reduction in 23 hours, from 10^2.5 to their detection threshold of 10^0.5, which I can't square with the 8.5 hour half-life. [Edit: it looks like I'm potentially confused about what TCID50/mL means?]
I also don't know how to compare their detection threshold with the point at which I should be willing to handle a cardboard box (with varying levels of cleaning and PPE). Is their test basically as sensitive as my immune system (in that I shouldn't handle something where they could see a viable virus, and can handle something where they can't)? Or should I be letting boxes sit for 3 days?
Worth noting that a lot of metal handles will be coated with a finish that prevents you from actually touching the metal. This is because these metals (especially copper) can leave a strong metallic smell on your hands which people typically dislike, and also because it prevents the metals from tarnishing. These handles will not help reduce infection and will need copper tape on them.
Killing bacteria isn't the same as killing viruses. Do we have reason to expect the same efficiency?
Sorry, forgot to modify this for a virus-specific claim, but yes.
On solid copper, H1N1 decreased by 4 logs in 6 hours in this review; vaccinia and monkeypox viruses were reduced by 6 logs in 3 minutes in this study; murine norovirus was destroyed in 30 minutes in this study, though it doesn't work very well at 4C; and another review says that copper oxide filters neutralize all of "bacteriophages [58-62], Infectious Bronchitis Virus [63], Poliovirus [61,64], Junin Virus [59], Herpes Simplex Virus [58,59], Human Immunodeficiency Virus Type 1 (HIV-1) [11,65-67], West Nile Virus [11], Coxsackie Virus Types B2 & B4, Echovirus 4 and Simian Rotavirus SA11 [68]. More recently, the inactivation of Influenza A [55,65], Rhinovirus 2, Yellow Fever, Measles, Respiratory Syncytial Virus, Parainfluenza 3, Punta Toro, Pichinde, Adenovirus Type 1, Cytomegalovirus, and Vaccinia [65]".
This ERI review concludes that there was really only one RCT (the one you linked), and they found that the study didn't actually reach significance
Our calculation found that the difference in the HAI rate (regardless of MRSA/VRE colonization status) between the study groups was not significant (copper-equipped ICUs: 17/294 [5.8%] versu snon-copper-equipped ICUs: 29/320 [9.1%]; p=0.123). The median length of stay for both groups was four days (p=0.74). The reported mortality rate was 42/294 patients (14.29%) in copper-equipped ICUs versus 50/320 (15.63%) in non-copper-equipped ICUs(p=0.64).
What's going on here is that Salgado splits outcomes into 4 groups, nothing, infection, colonization, and both, and finds a difference between the 4 groups. The review says "I only care about infection" and compares infection vs non-infection, and finds no significance. Each version of their math checks out, but I'm inclined to trust the review here.
This quasiexperimental study found similar decreases in infection rates however.
I'm not sure how to evaluate this evidence, but I'd be cautious about taking the Salgado results on its face.
Earlier I heard something like "wrinkles in the copper can reduce the effect, something something the fluids get caught in little pockets and leave spots that don't touch the copper."
Have you heard anything about that and have any thoughts on that? A lot of the images I see of people coppering their doorknobs are particularly wrinkly, and I'm wondering how much effort to put into getting everything smooth.
Not that it's necessary to make this comment complete, but I'd love to hear more about that 50% estimate. I've had a very hard time getting data on that.
Do you expect this to work for copper that has oxidized? Our bathroom copper is turning green and not sure if it's still doing anything.
The document referring to copper that I found via SSC was https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3067274/ .
The time of contact killing listed among the different microbes ranges from 1 minute to over a week. I don't know which example of a microbe would be closest to copper.
One big problem that may exist with using copper that I came across is that copper may reduce in efficacy if it is frequently cleaned, whereas stainless steel is fine to repeatedly clean. Source
The cleaner suggested to be used on copper surfaces without reducing its effic...
Is there a reason we're not spamming reddit/discords etc. with this advice?
I don't have enough karma on reddit to do things, but r/china_flu, r/lifeprotips, r/todayilearned all seem like good places to post this information.
Additionally, it might be worth it to spam amazon listings of copper tape with reviews saying it has antiviral properties. Possibly contacting the sellers of the tape as well.
Living in a group house? Consider copper tape on:
Front door handle
Bathroom door handle and sink handle
Refrigerator Door handle
Kitchen trash lid handle if not touchless
Microwave handle + small square of cutout copper tape on '+1 minute' microwave button
That seems useful. You forgot one of the most commonly touched items - phones and computers. I am gonna put tape on the back of my phone case and my laptop.
This is a good point, but for what it's worth I don't fully endorse coppering your phone (mine isn't coppered). Several people have anecdotally reported it being uncomfortable or irritating on their hands, or receiving tiny cuts from the copper, etc.
Absorption through skin is incredibly low, but I do take the risk of open (if tiny) hand wounds seriously, and also generally try to reduce my total copper contact in case anything weird does happen, since this is not tested by time.
But if you are constantly handling your phone it will reduce the value of frequent washing/sanitizing of hands, since anything you do get on your hands will transfer to your phone.
Although, I don't know what the numbers look like for transferring virus when a touch occurs -- e.g. if we look at a path like "handshake -> touch phone -> [wash hands] -> touch phone -> touch face", how much of the virus is left after four sequential touch events like that? Perhaps this kind of secondary contamination is not actually a huge deal? I have no idea.
Edit: Sounds like this isn't very useful because you'll be able tell if you're having trouble breathing? See comment below.
Advice: Get a pulse oximeter to be able to triage at home.
Reasoning: If you're mildly sick, you probably don't want to go to a medical office (both because you'll be clogging up an overcrowded system, and because you'll be around people who are even sicker). But you need to know when you're sick enough to need medical care.
One way medical professionals triage is by vital signs. Most of them are obvious either to you or to other people (shortness of breath, paleness, dizziness, turning blue) but oxygen saturation (how well-oxygenated your blood is) is not. If you think you might have pneumonia (one of the common effects of coronavirus), low oxygen saturation is one of the things that would indicate that, and lower numbers should move you toward getting medical care. 95% and above is normal (at sea level) and lower numbers mean it's likely your lungs aren't working properly (with outcomes being worse the lower the number is).
The device is cheap and easy to use.
Note that you might still be very sick and need medical care even if your oxygen level is fine, so this is a way to rule in being sick enough to need medical care but doesn't rule it out.
Guide to using and what levels are normal
More detailed instructions for troubleshooting
Article on lower oxygen saturation meaning worse outcomes for pneumonia
(I'm not a medical professional and would appreciate it if someone who is would double-check the logic here, or some risk I'm not thinking of in terms of people reading it wrong and coming to wrong conclusions)
TL;DR. If you have (slightly) low PaO2, but no trouble breathing, you probably don't need to go to the hospital. And if you have trouble breathing, you should probably go to the hospital whether or not you have low PaO2. So testing for oxygen saturation doesn't add much.
I had an online conversation with an intensive care physician. I sent him a translated version of juliawise's text and he said he didn't think buying the pulse oximeter would help and then sent me a 5 minute audio explaining why. The following text is his audio translated from Portuguese to English, I hope there are no wrong translations and I changed my mind after listening to him. Please also share what you think about his response:
"All pneumonia will desaturate the patient. O2 saturation is related to perfusion (gas exchange). Patient with acute respiratory syndrome (inflammation of the lungs by viral or bacterial infection) may course with poor tissue perfusion, that is, inadequate tissue oxygenation. One way to evaluate this is pulse oximetry, PaO2.
Patients with respiratory discomfort due to lung inflammation may or may not present desaturation. PaO2 < 90 indicates oxygen therapy. ...
This comment could maybe use a tl;dr saying:
If you have (slightly) low SpO2, but no trouble breathing, you probably don't need to go to the hospital. And if you have trouble breathing, you should probably go to the hospital whether or not you have low SpO2. So testing for oxygen saturation doesn't add much.
Is there any info the comment was meant to convey that that leaves out?
There seems to be a general variance in what pulse oximeters display when measuring healthy individuals with readings from 94% - 100%. I also seem to remember reading that they are sensitive to altitude, whether hands are cold etc (n.b typing on phone, can't verify at the mo)
Talking to a doctor friend -- in clinical settings if an oximeter shows a reading < 90%, it's considered serious, but different people respond differently, but closely enough for the purposes of this discussion to fall into two groups. Either you develop a shortness of bre...
It seems to me that the usefulness of a pulse oximeter depends on the progression of the disease. If "low osat" comes before "fever etc", then a pulse oximeter would help you move from "low osat → fever etc. → see a doctor" to "low osat → see a doctor → fever etc.". But if "fever etc." comes first, I would think you would be at "fever etc. → see a doctor → get osat measured" regardless of whether you have a pulse oximeter, and so I don't see how the p...
This is useful in case you have facing a choice of riding it out at home and going to a hospital with high probability of getting infected if you're not already. E.g. if you have fever chances are still high you're just experiencing regular flu, and should not go to the hospital, but if your oxigen starts dropping into the danger zone you need to go.
This site provides link for medical kit. You can copy and paste the supply list rather than purchase, or follow link to each item.
The logic is to "save you a trip to the doctor, or to support remote care via phone/video chat. " Recommended diagnostic tools are digital thermometer, finger oximeter, blood pressure cuff, and stethoscope for lung sounds.
In order to avoid cross infection, it is a good idea to use telemedicine rather than emergency room or doctors' offices.
Suggestion: research options for video chat, text messaging, or emailing d...
You should have some kind of electrolyte powder or electrolyte drinks on hand. When sick with any disease that can cause a fever (Fever is one of the symptoms of COVID-19 that pretty much everyone gets), staying hydrated is possibly the most important thing for you to be doing. You may be losing fluids from sweating and you may not be paying much attention to how much you are drinking. You will do a better job staying hydrated if everything you need to be hydrated can be right next to your bed. Once you have a fever it will really suck to go acquire stuff and you should be staying at home anyway.
Don't bother with the drinks. Recommended home-made rehydration drinks usually are sugar + salt for electrolytes. You want ~12x as much sugar as salt, and if you want to prep early, you can store the sugar-salt mixture and add it to water - you want about a half tablespoon of the mixture pur cup of water.
https://www.wikihow.com/Make-an-Oral-Rehydration-Salts-Drink-(ORS)
Unless this is the only thing you have to eat/drink for more than a couple days, this is fine - no need for anything complicated or expensive. And if you're too sick to eat solids or other foods, I'd suspect you don't have COVID-19, you have something else.
Can you respond directly to the claims that potassium and magnesium are also useful? It seems like your implicit model is that people will definitely be able to eat and therefore those will not be a concern.
Hospitalization and oxygen therapy thresholds
Tl;dr: Not knowing much about this and not a doctor, my current policy is to go to a hospital if SpO2 drops below ~92% and my hospital isn’t completely overrun, unless my SpO2 is naturally low or some other extenuating circumstance. If I was forced to use an oxygen concentrator outside of a hospital, I would target a ~~94-96% SpO2 range, trying very hard to make sure I didn’t hit 99%
If you do have COVID and shortness of breath, when do you go to a hospital?
Hopefully you already have a pulse oximeter as Julia Wise recommends. But sources say anywhere between 90 and 95% SpO2 is the threshold for hospitalization (WHO says <= 93% is classified as severe, ctrl+f “O2”), while other sources say you should threshold on trouble breathing and shortness of breath, not the actual SpO2 number.
It seems to me that using “trouble breathing” as the indicator would track the lung blockages and thus immune response relatively well, while O2 as an indicator would track the danger metric directly (if in fact the primary source of death is insufficient oxygen; if anyone knows this, would be useful).
The benefit of looking at trouble breathing is that it’s an advance indicator. Usually people progress from oxygen therapy to ventilators relatively quickly. If you have naturally low SpO2, your O2 might drop under threshold (say, 93%) in the early stages with mild trouble breathing, but you wouldn’t have much of a dangerous immune response until later. In this case, you’d have wanted to use difficulty breathing as your indicator instead of SpO2.
That being said, having low oxygen seems pretty bad for you, both by common sense and science. For example, 92% or lower is associated with increased morbidity in pneumonia patients; <90% is increased with 36% increased morbidity. Since it’s hard to measure even moderate effects due to the treatment-correlated-with-severity issue, my guess is that there’s some general bodily harm from reduced oxygen even at levels like 95%, though I don’t know how much. So at some SpO2 threshold, I think you want to be supplementing oxygen even if your breathing doesn’t feel that difficult.
Unfortunately, it seems like you can’t supplement oxygen at 95%, because over-oxygenating causes neuronal damage. Standard targets appear to be 94-98% or 92-96%. This study says it seems bad to set your target range during oxygen therapy to greater than 92-96%, because one inevitably exceeds the upper target occasionally. This review/musing muses that it’s a difficult problem, evidence for hyperoxaemia being pretty bad is “comparatively strong”, but not strong enough to warrant especially conservative oxygen titration. Because of these numbers, I think 92-93% is a reasonable threshold to self-hospitalize, since anything above this means they probably shouldn’t be oxygenating you anyways.
If hospitals are overloaded and you have to do oxygen therapy yourself (really try not to do this), I think the targets above are still reasonable, subject to your ability to titrate well with the machine. If you have lots of trouble, of course be conservative. However, you may be able to do better than hospitals: the first study above says that “even in a research setting in the intensive care unit, in which patients receiving mechanical ventilation are closely monitored, most patients who were randomized to an SpO2 target of 90–92% and were receiving supplementary oxygen did not have their inspired oxygen reduced if the SpO2 was 99% or 100%.” So—seems like you could easily do better monitoring than this if you were oxygenating at home. This is why I would probably shoot for 94-96% myself.
Hand sanitizer is becoming hard to find. Here are some WHO guidelines on making your own :
https://www.who.int/gpsc/5may/Guide_to_Local_Production.pdf
Formula 1:
• Ethanol 96%: 8333 ml • Hydrogen peroxide 3%: 417 ml • Glycerol 98%: 145 ml
Formula 2:
• Isopropyl alcohol 99.8%: 7515 ml • Hydrogen peroxide 3%: 417 ml • Glycerol 98%: 145 ml
Edit: Top off with distilled water until you get 10L of product.
My justification is argument from authority. I have no explicit model. Although both formulas use high concentrations of alcohol which are known to be effective disinfectants.
(FactorialCode has fixed it.)
The formulas above are incomplete. You have to fill them up to ten litres with water. Thus it is written in the PDF.
(As far as I know, too high an alcohol concentration makes the sanitizer less effective.)
If 99%+ isopropyl alcohol becomes unavailable, it looks like the other common concentrations are 70% and 91%. Using 70% isopropyl alcohol and not diluting gives you 65% alcohol, which is below the 75% in the recipe-- anyone know if 65% is likely to be effective?
Hand sanitizer is a poor substitute for actually washing your hands with soap and water.
Coronaviruses are "enveloped" viruses, which means they have a fat-based shell that protects the genetic material and (presumably) aids it in infecting a cell.
Destroying this shell "kills" the virus.
While an alcohol sanitizer can of course dissolve the fats in the shell, it is difficult to get enough alcohol all over the skin to do this.
Soap is more effective because it actively attacks fats, and of course washing your hands provides far more volume and time in which to destroy the virus shells.
Normally something with AfA as justification would be moved to comments, but it's useful and extremely specific in ways that can still be the foundations for a good argument, so we're leaving it in answers.
I feel like citing WHO is just about as valid as it gets in this context. WHO is just as much "from authority" as citing a few scientific papers.
The aim of your quarantine procedure and other actions should be to delay your exposure to coronavirus until after the peak has passed. It is unlikely to be possible to delay it indefinitely, especially if we are going to have a return to normalcy.
With every epidemic there is likely to be a peak - a period of exponential growth, climaxing in a peak and then a slowdown. Your goal should be to get exposed after the peak period. During the peak, medical supplies will be stretched very thin and hospitals may be overflowing. After the peak, medical professionals have a lot of experience dealing with the disease and we will know the landscape of outcomes and treatments. As long as the medical systems are not destroyed by the virus, that may be the best time to get it.
I modeled a logistic growth equations for a population of 7 million (bay area) and different estimates of the doubling rate I found in the literature - for a doubling rate of every 3 days, the peak seems to come after about 2 months from initial exposure. For a doubling rate of every 7 days, the peak comes about 4 months after initial exposure. Since the virus has likely been circulating for several weeks already, we can predict the peak in the bay area is 1-3 months out. How it actually plays out will vary a lot based on containment measures, public events, lifestyle of the populace, etc.
This is all extremely speculative but gives me a goal to shoot for - before I was trying to figure out what is the goal of quarantine for myself, if I was ever going to rejoin society. Now I have a model for why I should avoid getting it.
Instead of a single peak moment, we want to think about "the time period during which medical supplies and services are overwhelmed with demand". And that starts, in my rough estimation, the moment all the hospital beds are full.
In the US, we have 3 hospital beds for every 1000 people, and 2 of them are occupied on average. So we're going to start having problems once 1 in 1000 people want to go to the hospital for coronavirus, which corresponds to an infection rate around 1%.
So that pushes the moment of great worry forward by quite a bit!
On the other side, it's hard to predict when supply will again overtake demand. Maybe governmental intervention comes through on a massive scale, maybe mass quarantine works, maybe the weather warms up and transmission declines. But I'm worried it will take months for any of those to happen after the crisis times begin.
I would modify your advice to "2 weeks before all the hospital beds are full (in your local region)", because 2 weeks is roughly the lag time between exposure and needing hospitalization (I think?). With exponential growth @ 5day doubling time, you really want to not catch it when 0.01%ish of the local population is hospitalized [assuming per-capita hospital beds in your region is typical of the USA]. My region has ~7M people, so I would be thinking about upping my social-isolation game when 700 people in my region are in the hospital, or something vaguely like that. Probably adjust that down quite a bit for uncertainty in the input parameters, and for not all cases being diagnosed (even in the hospital). Adjust down even more if lots of hospital staff are likely to get sick or quarantined because they're not taking appropriate precautions, which seems probable at the moment.
[EDIT: enough has been learned since I made this model that it is now deprecated. I am now working from home, indeed 2 weeks after the answer was first composed]
A guesstimate model I made to determine whether I should stay home from work. Most of the innovation is in collecting guesses/gut feelings and then doing the calculations. Based on my guesses, I shouldn't bother working from home for a few months. [EDIT: for complicated reasons it's probably more like one month] [EDIT: after further adjustments, partly to parameters and partly to the structure, it's now like 2 weeks] https://www.getguesstimate.com/models/15212
Meta note: the costs of being isolated are roughly linear in how long you're isolated, but the costs of being in public are exponential in the regime where your chance of getting infected is small and proportional to the number of people who are infected. As a result, you'd rather self-isolate one week early than one week late. Given the model uncertainty in any modelling attempt like this, this means you probably want to be a bit more paranoid than the model suggests.
Model update: previously, the model wasn't including the possibility of a chain of length more than 1 of people infecting each other at work, ending with you. This increases the disease burden of attending work by a factor of 2.
Guesstimate model update: Number of days you want to wait until working from home is (unsurprisingly) very dependent on epidemic doubling time estimates. Fiddling with the distribution to basically update on reports of 1- or 2-day doubling times in some contexts, the model now says that I want to wait a month before working from home.
A non-obvious flaw in the model: the "number of days until you should work from home" distribution is using in its calculation samples from the "current dollar value per day of disease burden of attending work", rather than the mean as it should. There's no easy way to fix this, but this pushes that number lower. Note that this error doesn't affect the calculation of whether I should stay home right now. [EDIT: but it does turn "wait a few months" into "wait a bit over a month"]
It looks like you're just assuming how many people will be infected, rather than basing that off current infection levels? Is that correct?
A 2 weeks supply of food sounds like far too short a supply. The first case of 'atypical pneumonia' was noticed in Wuhan in late Dec. It is now late Feb. They have by now organized themselves in Wuhan to the point where all of the ill people are getting sent to 'local' (temporary) 'hospitals' and the 'local hospitals' are triaging and sending seriously ill people onto actual hospitals with the capacity to care for people who are seriously ill (like requiring oxygen). But this level of organization is a fairly recent situation. Even 2 weeks ago, sick people were literally walking to hospitals, because ambulances were swamped; they were being turned away from hospitals for lack of beds and supplies, and medical personnel to look after them; they were sitting in hospital waiting rooms for hours being cross exposed to other sick people, etc. So, even with massive efforts on the part of the government, it took about 2 months for them to get their act together in a real hot spot of infection. If you are unfortunate enough to end up in a similar type 'hot spot' to Wuhan, (but still live in a first world country) it probably won't take longer than 2 months for the government to get its act together, but I wouldn't assume they will do much better than that... so, if you are planning on buying a little insurance, I'd suggest that a 2 month supply of food, etc, is about minimum of what you would need to get through a (1st world) worst case scenario, rather than 2 weeks.
And a 3 months supply would probably be a better choice than a 2 month supply. It's not like Wuhan is virus free or anything close to it, today, 2 months in...
A 3 month's supply of food sounds crazy, and, true, you probably won't need it. But, it's almost cost free to supply yourself with it. No one at all is suggesting power outages. So, you can probably just stock up on food and supplies you normally use anyway, at least for frozen, canned, and non-perishable type things. That obviously won't do for stuff like milk and fresh fruits and salad stuff, so you'll have to make some substitutions there, but for most other stuff you should be OK if you just buy extras of things you normally buy anyway. The only cost is the inconvenience of buying it all at once, and finding a convenient place to stack it down until you need it.
I have read many reports from people in Wuhan and there is food in the grocery stores. Actually it seems like no currently effected area has a permanent food shortage - there is a run on the stores and then they are full after a restock. However, shopping requires you to leave your house so you will want to minimize it. I think people are over-focusing on food shopping because it feels actionable. You are right that there is almost no downside
If one becomes ill, he needs foods which he could eat without cooking and which are very nutritious. For around one month. One can't eat raw rice, but dry bananas are great.
Cabin fever is unnecessary.
According to the CDC the coronavirus is thought to spread similarly to how the common cold spreads: person-to-person spread, and contact with infected surfaces or objects. There are certainly ways to get out of the house without coming in close contact with other people and without coming into contact with surfaces that others have touched. For example, going for a walk or a bike ride. (In densely populated cities this will certainly be harder.)
Furthermore, socializing with friends who you trust shouldn't be too risky. From the CDC:
People are thought to be most contagious when they are most symptomatic (the sickest).
Some spread might be possible before people show symptoms; there have been reports of this occurring with this new coronavirus, but this is not thought to be the main way the virus spreads.
So then, if you know/trust that your friends are asymptomatic, and you trust that they are hygienic (wash their hands, wipe their counters, etc.), socializing with them shouldn't be too risky.
If it spreads like the common cold, how worried should I be about kissing people? Reason:
Kissing does not efficiently spread cold infection ... Of 16 susceptible recipients, only one became infected by a one or one-and-a-half minute kiss with an infectious donor.
Source: https://journals.sagepub.com/doi/pdf/10.1177/014556139407300906
Does anyone have an update/ thoughts, on how safe it would be to take walks with asymptomatic friends one on one and keeping a distance of about 6 feet ?
Recommendation: cover the back of your smartphone in copper tape.
Reasoning: in addition to the reasoning for putting copper on all commonly touched surfaces, your phone is an especially good choice because of the "copper halo effect", in which copper ions move from copper surfaces to nearby surfaces (like, say, your hands), leaving them much less hospitable to microbes. [Edit: As MalcolmOcean points out, this mechanism for the halo effect isn't supported by the Wikipedia page below. I made a leap to this explanation without realizing it. That said, I do think that copper (and copper oxides) will get on your hands as a result of this tape, partly because I've seen my hands turning a bit blue.]
https://en.m.wikipedia.org/wiki/Antimicrobial_copper-alloy_touch_surfaces
A downside is that your hands may turn slightly blue. [Also: See the comment below about uncertainty about how much copper you'll eat as a result of this; tldr: I don't know but I think it's probably fine]
[This is a signal boost for Lady Jade Beacham's response to Connor_Flexman, but the idea was originally introduced to me by James Payor]
Note that this can act as a Faraday cage around your phone and potentially reduce your reception.
With the fullback of my phone covered in copper I got ~0.2 Mbps on 4G. When I removed a 1 in.² on the upper left (where the antenna is on a Google pixel 3) it went up to 13 Mbps.
I assume having everything except for a small square covered is still pretty good, so I'm doing that.
Huh. This is quite important if true. Can anyone with a bit more physics/chemistry knowledge give an estimate for how long this will last on your hands, and how much coverage of your hands you will get? If this is a significant effect, it seems like a pretty useful piece of prep (copper on phones) that I am only just hearing about.
The halo effect (section on wikipedia) didn't seem to me to be about ions... I figured it was just like how if we're nearby & I'm less likely to get sick, then you're less likely to get sick, separate from my sickness having any effect on your immunity.
A thing I probably haven't thought enough about is, "how much this will impact your rate of copper ingestion, and is that very bad?" My guess is that this is less important than the effects on infectious disease; it seems like it would need to increase your copper consumption by 100x in order to produce major negative health effects (https://www.atsdr.cdc.gov/toxprofiles/tp132-c2.pdf). I may try to be virtuous and do a fermi on this later but also I'd welcome someone else trying to do it.
Edited to add:
The most obvious effect of having too much copper is ga
...I would much rather rinse a mobile phone regularly if it is water-proof (an increasing number is!) than use copper tape, although I would not use soap on the screen, to preserve its oleophobic properties; alternatively, if I were in a very susceptible group or if the virus were much more dangerous to me, I would find it more effective to put the phone in a plastic bag and either exchange it often or wash it as often as my own hands.
The thought process here is that copper tape cannot be applied to screens, which can end up very close to faces, but washing with soap is effective.
Maybe we should put copper on our hand sanitizer bottles. But does it take effect quickly enough to matter here?
Advice: Apply lotion after washing your hands.
Reasoning: Heavy handwashing can dry out your hands, which can lead to cracks forming, which are more vulnerable to infection. You can fight this by applying lotion after washing your hands.
Sources: have experienced dry hands -> cuts personally, a dermatologist told me it was a vulnerability.
Related: CDC recommends washing with warm or cool water as opposed to hot, because hot water doesn't help more and is more likely to bother your skin. https://www.cdc.gov/handwashing/show-me-the-science-handwashing.html
A discussion / recommendation on handwashing versus sanitizer would be most welcome, I think. I have seen recommendations ranging from "always wash hands if possible, use sanitizer only if handwashing is not possible" to "use hand sanitizer unless your hands are visibly dirty, in which case wash them."
I am a bit concerned that applying lotion after handwashing is potentially a good way to re-contaminate your hands, unless you and everyone in your household is very careful about how you handle the lotion.
(I seemingly managed to give myself irritant contact
...Their advice for healthcare settings is to prefer hand sanitizer, because it's better at killing germs, it doesn't dry your skin as much, and you're more likely to actually use it. https://www.cdc.gov/handhygiene/science/index.html
Their advice for community settings is to prefer soap and water, as far as I can tell because you're more likely to have stuff on your hands (grease, dirt), and because kids might drink it. https://www.cdc.gov/handwashing/show-me-the-science-hand-sanitizer.html
This coronavirus-specific page seems to treat them interchangeably. https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-prevent-spread.html
If the local case rate is not yet high enough to warrant quarantine, and you're hosting or attending events, then in addition to asking people to not come if they are sick or coughing, you also might want to implement fever screening.
Three studies of nCoV symptoms cited here found fever in 83%, 98%, and 98.6%. Studies are less precise on the exact timing of symptom manifestation, but fever appears to show up early. To screen people for fever, you need either an oral thermometer plus disposable probe covers, or a contactless infrared thermometer. A contactless thermometer is faster, but less reliable; if you use one, you will want to also have an oral thermometer plus probe covers to deal with false positives.
What temperatures should be used as cutoff when doing fever screening at events in the evening?
For me personally, self quarantine seems pretty unnecessary at this point, but I would act differently if I were in a different age group. Given the below death rates I would self quarantine if I were over 40. I would like to note I expect these death rates to be somewhat high because they are largely based on confirmed cases, which I expect to be disproportionately the worse cases that ended up in hospitals.
There was one case of Covid-19 in Solano county (CA) that couldn't be traced directly to travelers, which indicates community spread may be happening and Covid-19 may be spreading in the bay area.
| Age | Death Rate |
| 80+ years old | 14.8% |
| 70-79 years old | 8.0% |
| 60-69 years old | 3.6% |
| 50-59 years old | 1.3% |
| 40-49 years old | 0.4% |
| 30-39 years old | 0.2% |
| 20-29 years old | 0.2% |
| 10-19 years old | 0.2% |
| 0-9 years old | no fatalities |
Given the below death rates
Note that while your personal survival is quite important, getting infected and surviving can have quite awful effects. We don't know what the long-term effects are like yet (because we haven't hit the long-term yet), but I won't be surprised if post-viral fatigue is common.
Being ill is also unpleasant, and you become a risk to your community, and especially any elderly people in your community.
Sources Death Rates https://www.worldometers.info/coronavirus/coronavirus-age-sex-demographics/?fbclid=IwAR3pUihF3LkUPfXJgJF_DR98NpOfPoma0rVCqkKuR7olmlZFkQm8aprVzec
Solano County Case https://www.davisenterprise.com/local-news/newly-diagnosed-coronavirus-patient-being-treated-at-uc-davis-medical-center/
Great table to offer. Might be good to also update on some related state. Males seem twice as likely as females to contract the infection (not positive here if that also scales with age or not)
Also, those with preexisting condition (heart, lung, other immune system taxing states) are also more likely to suffer more, and be among those dying than those who are generally healthy.
I think there was also a suspected link between smoking and higher risk if exposed to COVID-19. That is probably too correlated with the other preexisting health conditions that might be too difficult to say much.
Note: I gave Finan a table using the new in-beta editor. Users in general still do not have editors available at the minute.
Consider that by quarantining yourself you're also protecting others from being infected (directly and indirectly) by you, some of whom may be in much higher risk categories. Given that we're still in the early stages of exponential growth, this seems quite significant.
Thanks for the useful data and advice for younger people! Please remove the long laundry list of recommendations at the end :)
Edit: Thank you. I will now fix your table.
Buying a bipap + O2 concentrator + capnometer + Y juntures + tubing can decrease chance of death given being infected by about a third.
Reasoning:
You probably need around 5L/min of 90% O2, which theoretically requires a medical grade condenser that requires a prescription. I, however, see no reason why getting 5 normal O2 condensers that can deliver 1L/min of 90% O2 and connecting them all with Y junctions won't work.
[Edit: you can probably do with 4L/min of 70% O2, so you'll need 2 O2 condensers. This advice is mostly based on priors and like 20 minutes of research. The crucial point is that you'll likely need at least 2 O2 condensers]
These devices should all be relatively easy to use. Many people use a bipap for sleep apnea. Many people with respiratory problems have their own O2 condenser that they use. The capnometer I'm less sure of, but there should be a simple flow chart on what to do. If there isn't, I will make one by talking to doctors.
The reason you need the capnometer is because giving people too much O2 also has its own host of problems.
Here's a model of the expected value of buying such a system for only 1 individual: (https://www.getguesstimate.com/models/15306)
This model assumes that there is 0 hospital capacity and it's only for 1 person. Model also doesn't take into account reduce quality of live because of the chance of chronic fatigue syndrome. Model also assumes 20% chance of getting COVID, which is pretty low. Disjunctions are more probable, so the value goes up rapidly with more people, but has a max because it can only be used on one person at at a time.
Bear in mind that the probability that a 2nd person you care about getting COVID conditioning on 1 person you care about getting COVID is pretty high because the people you care about hang out together.
The total cost is about 2k for the bipap, 5 * 400 for the O2 condensers, and 1k for the capnometer for 5k total.
If you think that more than 10% of the world is going to get COVID, buying 1 such setup for like 20 people is an obviously correct move given the model.
Things to watch out for: cheap chinese models of both of these devices.
Edit: took Daniel Filan's suggestion of adding Y juntures and tubing to the first line.
Do you have any thoughts on where to buy a bipap and a capnometer? Can you get them without a prescription? Are they sold on amazon? If you or anyone else manages to get this to work (or even just starts buying supplies for it), I'd love to know where they obtained all their supplies and what they ended up needing.
I guess people also need to buy Y junctures and tubing? If so, worth putting that in the first line IMO.
Hi Mark and others, thanks for sharing this info. Two questions:
1. When using the O2 concentrator, can we test for oxygen levels using Pulse Oximeter instead of capnometer? Looks like we need a prescription to buy a capnometer.
This paper finds that "During PSA in adults breathing room air, desaturation detectable by pulse oximeter usually occurs before overt changes in capnometry are identified." :
https://www.ncbi.nlm.nih.gov/pubmed/20880431
So, a pulse oximeter should suffice?
2. In the WHO report, they say: " About a quarter of severe and...
There is a 5% chance of getting critical form of COVID (source: WHO report)
That's a 40-page report and quickly ctrl-f:ing "5 %" didn't find anything to corroborate your claim, so it would be helpful if you could elaborate on that.
Open Source Hardware guide for coronavirus
https://coronavirustechhandbook.com/hardware
Hand operated ventilators
https://www.notechmagazine.com/2020/03/open-source-breathing-ventilators-covid19.html
Mark - any thoughts on producing a system like this in crazy scale (say 10-100K/month) for altruistic purposes (i.e., to save lives not to make money)? Please DM me if you'd be willing to discuss.
(EDIT: ignore this paragraph, it's not true) I've seen this discussed on another forum. Apparently, medical grade condensers require the patient to be put in a pharmacological coma so that their body doesn't fight all that air being shoved down their lungs. Makes sense since usually only stuff that's potentially harmful requires prescription.
Also, I've seen open discussions in at least one democratic country of confiscating privately owned condensers for the public healthcare. So if you end up buying some equipment, you will want to keep your mouth shut and perhaps use cash if possible.
If you develop a dry cough, do take cough drops and sip liquids to prevent yourself from coughing.
Reasoning: I've seen one doctor claim this is helpful because one of the causes of severity is how deep into the respiratory system the virus is able to travel. Apparently lower respiratory infections are more severe because the immune system has a harder time fighting it. Coughing tends to drive the virus deeper into the respiratory system.
When getting restaurant takeout or delivery, put the food in an oven and bake at at least 70C/160F for 30 minutes to kill the virus. To minimize contamination, I put the whole package containing the meal into the oven, wash my hands, then operate the oven. (This assumes that only the packaging and outside of the food is likely to be contaminated, because the inside is hot enough to kill the virus already. If this is not true for the meal you're getting, increase the oven temperature or time enough to thoroughly heat the food to 70C for 30 minutes.)
This also works for mask reuse (which is where I got the idea from originally). (This article says "The new coronavirus is sensitive to heat. It can effectively inactivate the new coronavirus by heating for 30 minutes at 56 degrees Celsius." but does not cite a source for this. I wasn't able to find a study for the COVID-19 virus, but did find the following data for SARS: https://link.springer.com/article/10.1007/s00430-004-0219-0/tables/1)
Thanks, this is a question I really wanted someone’s numbers on!
You said 70C for 30 mins, then said it again but I thought you were going to say a more extreme quantity the second time. Was that intentional?
I just thought of this idea: carry a box of disinfectant wipes everywhere, and whenever you want to touch a surface that's touched by many people (handrail, door handle, elevator button, touchscreen kiosk...) give it a quick wipe-down first. That protects you, helps protect other people, shows them how to do the same, and also disinfects your hands many times a day. Any problems with this?
Figure out now who will take care of you if you get extremely sick and who you will take care of if they get extremely sick.
Making these expectations explicit could pay off. Different people have different norms around what level of care vs avoidance should happen when someone is sick. If you became extremely sick, you might lose the coherence necessary to arrange help for yourself.
Work out at home instead of at the gym.
According to the CDC the coronavirus is thought to spread similarly to how the common cold spreads: person-to-person spread, and contact with infected surfaces or objects. The gym is a place where you'll be in close proximity with other people, and where you'll be touching surfaces that many other people have touched, and thus is a place where the risk of getting infected is high.
On top of that, the downside to working out at home seems quite low. There is so much that you can do without gym equipment (burpees are awesome if you don't mind the intensity), and there are large diminishing returns to exercising more and to exercising more efficiently. Plus, changing up your routine is good for both effectiveness and for fun.
How to exercise with dumbells to hit all the major muscle groups.
Another great resource for those without equipment:
Advice: have disposable wipes by the front door and use them to wipe your smartphone and then manipulate your handwashing sink each time you arrive home.
Model: You are touching your smartphone while out, and to whatever extent possible you want surfaces inside your home to be controlled. CDC recommends disinfecting touchscreens but many people don't because disinfectant can damage special coatings. One can bite the bullet or consider adding on another screen cover.
I have been disinfecting my smartphone and glasses with disinfectant wipes, and have had no problems with coatings so far. I haven't used them on my computer screen; I know the antireflective coating on the macbook screens can be sensitive.
My disinfectant wipes are neither alcohol nor bleach, but quaternary ammonium (with a list of ingredient names all having the form "...yl ammonium chloride".) My sense is that this seems to be typical of generic "disinfecting wipes".
I started to self-quarantine from 25 January, reasons: uncertainty in mortality and the need of a test run. At that moment the situation with mortality was not as clear as it is now. I still don't exclude higher mortality level (than in the table) as for many patients the disease is around one month long and this data is not accumulated yet. I also more than 40 years old and have hypertension which is a risk factor.
My observations about self-isolation: I eat more, and as a result my stockpile is going quicker than I expected. And also I gained weight. Also, sometimes I feel my self like in a prison and want to go out despite any risks. After I go out eventually, I felt more tired as possibly first sign of atrophy of muscles. All this means that long term self-isolation has its own risks, mostly cardio-vascular and mental state.
This test-run of self-quarantine helped me to perfect protocols of cleaning things after I went out and of proper wearing masks. Not all masks fit equally well, and it depends on the shape of the face.
What are the benefits of "don't go outside at all" vs "don't take walks, if you make sure to never be within 10 feet of people?" (I suppose how achievable this is depends on where you live. I guess I couldn't do it in NYC, but could do it in Berkeley easily)
I used to think CDC recommendations were not great but better than nothing. I've changed my mind after seeing them say coronavirus can't survive on surfaces for very long, so I'm retracting this comment.
I wonder if ensuring one has an exercise plan (or perhaps some equipment -- could be DIY type equipment) should not also be on the list of items to "stockpile" if one is self-isolating or even under quarantine.
I never really thought about that before you mentioned it, but I have an orbital machine in my workshop/garage so take that from granted.
I think you should try to get antibiotics, antivirals, and/or antifungals for secondary infections in case hospitals are full and you need to treat yourself. According to this study, “When populations with low immune function, such as older people, diabetics, people with HIV infection, people with long-term use of immunosuppressive agents, and pregnant women, are infected with 2019-nCoV, prompt administration of antibiotics to prevent infection and strengthening of immune support treatment might reduce complications and mortality.” About what treatment people in Wuhan were given, the study says:
Most patients were given antibiotic treatment (table 2); 25 (25%) patients were treated with a single antibiotic and 45 (45%) patients were given combination therapy. The antibiotics used generally covered common pathogens and some atypical pathogens; when secondary bacterial infection occurred, medication was administered according to the results of bacterial culture and drug sensitivity. The antibiotics used were cephalosporins, quinolones, carbapenems, tigecycline against methicillin-resistant Staphylococcus aureus, linezolid, and antifungal drugs. The duration of antibiotic treatment was 3–17 days (median 5 days [IQR 3–7]). 19 (19%) patients were also treated with methylprednisolone sodium succinate, methylprednisolone, and dexamethasone for 3–15 days (median 5 [3–7]).
I think this sort of treatment might be one of the biggest factors in lower mortality for people with access to hospitals, so I suspect that getting your hands on some prescription antibiotics beforehand could be quite valuable. Some of the pharmacies that Wei Dai recommends here could be good bets, though I'm still currently trying to figure out what the best way is to do this—if anyone has any ideas let me know.
This not-particularly-reliable source says "So far, there have been very few concurrent or subsequent bacterial infections, unlike Influenza where secondary bacterial infections are common and a large source of additional morbidity and mortality".
Check the active ingredient of your hand sanitizer. You may have one that contains benzalkonium chloride, which does not work against at least one type of coronavirus. (This turns out to be the case for one of the hand sanitizers I've been using.) Get one that has "greater than 60% ethanol or 70% isopropanol" instead, as recommended by CDC.
ETA: I didn't bother to check this until today, because why would the FDA approve or fail to pull from the market, hand sanitizers that don't work against an important group of viruses? And why hasn't there been any articles in the MSM about this?
That study is on inanimate surfaces, and benzalkonium chloride is the main ingredient of Clorox, Lysol and other disinfectant wipes. So it might be a good idea to switch to isopropanol wipes for surfaces too.
I'm pretty sure this can't be correct--they claim benzalkonium chloride has zero effectiveness, which is less than plain water! I think it has to be a data entry error.
This review cites some other studies that show benzalkonium chloride to be comparable to other disinfectants, although alcohol is still best by a considerable margin.
Do cardio exercise—at home or jogging (not gym for transmissibility reasons, as mentioned in this other answer.)
Why cardio, and why now? My thinking is: a primary reason for COVID hospitalization is not being able to get enough oxygen (cf this answer), and its primary treatment is with concentrated oxygen or (in more severe cases) mechanical ventilation, and the nightmare scenario is not having concentrated oxygen equipment etc. for the number of people who need it (I guess some appreciable fraction of the 20% of cases that require hospitalization). So it seems highly plausible to me that starting from a state of good cardiovascular health (hence high blood volume, high lung capacity, efficient heart pumping, etc.) would give the body some extra slack such that COVID can gunk up the lungs slightly more and for slightly longer, before you suffocate and die. This speculation is also compatible with the COVID death rates being apparently higher in populations that I would guess have generally worse cardiovascular health (in terms of age, pre-existing conditions, etc.). Again, to be clear, I have no proof of a causal connection, or even proof of correlation, just a vague suggestion and plausible-seeming mechanism (to my non-medically-knowledgeable mind).
By the way, my experience is that, after a long exercise hiatus, there's clear improvement in "not feeling out of breath" over the course of even the first couple weeks of cardio exercise, so it's not too late to get started. :)
Here's my personal tips on (what I find to be) a practical and sustainable home cardio exercise routine, and injury-free jogging. Also see comments on this answer.
In the worst case that it does nothing to help with COVID, hey, starting an exercise routine is still an awesome idea for mental health, longevity, etc. :)
(PS: Don't overdo it, I hear overtraining is counterproductive.)
Just saw this thread on a subreddit for medical professionals suggesting this could be a bad idea:
https://www.reddit.com/r/medicine/comments/fmvbtc/could_highintensity_exercise_increase_severity_of/
Update March 4
I've done an extensive analysis of the disease and Impact of a Pandemic. http://tinyurl.com/sv5v4vc
I'll excerpt my On Masks Section as I suspect the reasoning contained within will be the most appropriate and interesting to this thread. But there is good stuff throughout, I've built things for lay readability, and am not a technical expert, I would appreciate thoughts and advice. I don't have variables for mask exposure, but I think my reasoning is solid and useful. You can tweet me @qastokes
About N95 Masks
All non-N95 face masks, such as medical masks, (of the dental kind), are relatively useless for self-protection, as they lack a seal. Please donate your excess to medical facilities. These are very useful for containing the spreading of all illness, those who are sick and coughing, regardless of disease, should find and wear these type masks. Containing spread is far more effective than reducing exposure for managing the risks.
Please understand N95 isn't prevention, it's odds increase. When properly fitted and used it reduces exposure, but technically it's only 95% efficient. An N95 might keep a doctor with constant exposure alive, but won't help Joe who's out shopping much. Wearing a mask could theoretically increase your risk if used wrong, by being a capture of virus that moves along with you and extends your exposure time. It is not generally helpful, compared with handwashing and effective prevention protocols.
It is true there is benefit to be had by using a mask. But it is only significant if you are competent in following the use protocol. It is better by far to learn & to carefully follow all the other higher impact protocols, especially handwashing. By far the greater benefit, for you individually considering your total exposure risk across time regarding the disease and it's spread, around you to managing your personal exposure will be for those managing the disease directly to have the best protection they can. Hence my advice to donate extra masks to those at highest risk.
Think about this along the lines of "the more the disease spreads, the greater your total exposure risk, regardless of managing your personal exposure risks."
Note: For really significant improvement in your exposure chances, I & wearing a mask effectively, you will need to carefully follow the behavior protocol for a disposable full body exposure management system. A protocol which includes gloves, a hooded tyvek particulate suit, and goggles, along with the mask, this is only really applicable in an extremely exposing environment. Additionally, a P100 would be the optimal mask of choice for this situation and protocol.
The biggest risk management benefit comes from one complete set of masks and a full body exposure management system for every one of your loved ones. This allows you the freedom to make one situation optimizing decision in a worst case scenario.
This would look like: The family is out of food. Healthcare is overburdened to the point the death rate has matched the critical cases rate. You must move with high risk of high exposure.
Alternately, with planning these suits can also be burned one use at a time in a clean room caring for a loved one, allowing for several days of constant and very direct care with low gain viral load & exposure risk for those still without symptoms or as yet uninfected.
Note for completeness: of all the routine contexts to wear a mask, high droplet spray environments are the ones the mask will help in the most, especially if you sanitize your clothes afterwords. I would strongly consider wearing one in a crowded subway, if there is a known outbreak in your city. This would only significantly help if you wear the mask correctly, sanitize clothes, & don't touch your face and are meticulous about hand washing.
Advice: Humidifiers. We need them now, and everywhere that people gather in temperate climates. There's a reason why the common cold, influenza, and indeed SARS all die out as summer approaches in seasonal climates--relative humidity over 40% is the best method for controlling airborne viruses.
Influenza season has been ending every spring, (https://journals.plos.org/plospathogens/article/file?type=printable&id=10.1371/journal.ppat.1003194) long before DNA tests, masks, or alcohol sprays. Humidity under 30% like we regularly encounter in buildings during winter occurs naturally very rarely. It degrades our immune defenses and increases the longevity of airborne viruses.
"The present study allowed us to assess viral infectivity under various levels of relative humidity and showed that one hour after coughing, ∼5 times more virus remains infectious at 7–23% relative humidity (RH) than at ≥43% RH." https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3583861/
"Low ambient humidity impairs barrier function and innate resistance against influenza infection" https://www.pnas.org/content/pnas/116/22/10905.full.pdf
Need to get the news out. I wrote a Medium article on it: https://medium.com/@crissmanloomis/the-end-of-the-covid-19-outbreak-d578092282c8
What's your model for how useful this is? COVID spreads in public places, and it's mostly spreading via droplets on surfaces. Changing indoor humidity seems like it would only have a very minor impact, if any.
This makes little sense to me. Viruses are different, spread differently, and will react differently to environmental changes.
And I do not understand why checking for fever routinely is less tractable as a routine habit than, say, using humidifers. And distracting from exclusively promoting handwashing seems like a huge net negative, given that we still haven't gotten people to change their habits.
It is almost 90 degrees in Singapore, and the humidity is almost 90 percent. and it spreads...
TLDR You may be able to use a rice cooker, instant pot or pressure cooker to sanitize disposable masks after wearing them, although this will slightly damage the mask.
Due to the worldwide mask shortage, it seems inevitable that many people are going to have to reuse masks. Personally I have 2 masks per member of my household which seems troubling low.
It may be possible to decontaminate masks - I found a paper that reviewed 5 mask decontamination methods, both a review of how they affected the mask, and a review of how effective they were at decontaminating. The papers are very technical, so please double-check my interpretation
Takeaway - here are the 5 methods in the first paper:
All methods of decontamination damaged the masks. It seems that alcohol and bleach significantly damaged overall filter quality (ratio 0.30 to original), but rice cooker and autoclave relatively preserved it (0.98 to original). I can't see the results for the IPA method on their chart but I expect it to be similar to the other chemical methods.
The other paper on sanitizing efficiency also looked at UVC and UVA light. It found "Bleach, UVC, an autoclave, and a <rice cooker> provide better biocidal efficacy than ethanol and UVA".
My conclusion in this is that rice cookers, pressure cookers and especially the instant pot - which offer comparable performance to commercial autoclaves can be used in an emergency situation to sterilize masks for a few uses. Be very careful about the way you don and doff the mask and handle them generally.
The CDC recommends using "...a cleanable face shield (preferred) or a surgical mask over an N95 respirator..." for extended use or reuse. This may make it more difficult to breathe, but perhaps worth trying. Surgical masks are also not so available these days, but maybe something like a bandana or other covering would also help protect the mask.
https://www.cdc.gov/niosh/topics/hcwcontrols/recommendedguidanceextuse.html
A lot of stores are using touchscreens now meaning you're touching the same spot as literally the entire flow of customers before you and no one ever cleans those. But you can use a touch screen stylus. I got one with a cap so that I can carry it more easily without contaminating other surfaces.
Advertise that you are seeing the smoke.
From the article:
As Eliezer reminded us, most people sitting alone in a room will quickly get out if it starts filling up with smoke. But if two other people in the room seem unperturbed, almost everyone will stay put. That is the result of a famous experiment from the 1960s and its replications — people will sit and nervously look around at their peers for 20 minutes even as thick smoke starts obscuring their vision.
and
The goal of this post is twofold. First, if you’re the sort of person who will keep sitting in a smoke filled room until someone else gets up, I’m here to be that someone for you.
If results of the experiment are real, I think we can expect 1) people to hesitate to take the coronavirus seriously, 2) people to take it more seriously if they know that you are taking it seriously. We want people to take it seriously, and so advertising that you take it seriously — as Jacobian did — seems like a good thing to do.
This could mean texting your family and friends, or posting on social media (in such a way that doesn't incite panic).
Consider that some people may be higher yield targets of your advertising than others. Someone who is capable of changing their mind, has the option of working from home and who lives in a densely populated area is an example of a high yield target.
Nutrition seems to have some influence on the effects of viruses.
Make sure you're not deficient in selenium or vitamin E. One brazil nut per day is enough to give you more than the RDA for selenium.
Note that selenium deficiency is relatively common in central China. The average selenium level in Hubei isn't low, but it has a large range of levels, and the person with the lowest level in that study was from Hubei.
There are also some reports that vitamin C might be valuable. But there's some concern that large doses of vitamin C are risky if you have high iron levels (usually measured by a blood test for ferritin).
I expect that nutrition has a pretty low probability of helping, but it also has a pretty low cost.
It is recommended to avoid touching your eyes, nose, and mouth[1]. People tend to inadvertently touch their eyes, nose, and mouth many times per hour[2]. If you think you can substantially reduce the number of times you touch your face by training yourself to avoid doing it, in some low-effort way, go for it. If it takes time to become good at not touching one's face, it may be worthwhile to start training at it now even if where you live is currently coronavirus-free.
--
[1]: The CDC (Centers for Disease Control and Prevention) writes:
The best way to prevent illness is to avoid being exposed to this virus. However, as a reminder, CDC always recommends everyday preventive actions to help prevent the spread of respiratory diseases, including:
[...]
- Avoid touching your eyes, nose, and mouth.
[2]: The video by the CDC that Davidmanheim linked to claimed: "Studies have shown that people touch their eyes, nose, and mouth about 25 times every hour without even realizing it!"
I haven't tried it, but there's a funny idea to stop touching your face by taping your elbows.
I've been trying to reduce my face touching for more than 6 months now as part of a project to get less colds and only managed to really get there in the last 2 months. I also work in a lab with gloves where I have to take care what I touch a lot, which is daily training. Still I have found it frustratingly hard not to do it, so I don't know if many people can quickly train themselves.
Things that help me:
I've managed to not bite my nails for the past ~3 weeks (longest stretch of my adult life!) thanks to that special kind of transparent nail polish that make your nails taste bad :-P
I shaved my beard. I've only had it for about 6 months, and I played with it constantly and unconsciously. Since shaving it off, I bet I'm touching my face 10% as often at most, and only fleetingly.
Social engineering-- ask your friends and family to tell you if touch your face. Do the same for others.
One piece of advice is to keep your hands below shoulder level when you are in public spaces to avoid the temptation to touch your face.
I discovered a way to practice this recently, I was drawing with vine charcoal, which is dark and very dusty, and I got dark dust all over my hands. Then I touched my face inadvertantly and I could see in the mirror where I had touched.
Later I tried to wash it off and was able to wash it off only when I really focused on how I moved my hands in order to scrub any area. The entire thing felt like good practice with hand higene. So to practice this, improvise a colored dust - charcoal, ash etc, and practice washing hands and not touching face.
If you have long(-ish) hair, wear something that will keep your hair off your face.
Rationale: I'm training myself not to touch my face, and more often than not, I want to do so to get my hair out of the way.
Also, I touch my hair very often (to fix its position) but I wash my hair much less than I wash my hands, so if my hair regularly touches my face, it's plausible that I'm at greater risk of catching the virus through my hair rather than through my hands.
It seems like you should never touch buttons outside your house with your fingers. Carrying around an object like a pen that's wrapped in copper tape to push buttons allows you to use buttons without touching them with your fingers.
When it's hard or impossible to avoid touching one's face or staying 2 meters away from others, wear a combination of ski mask, safety or medical goggles, and surgical mask. This would prevent touching one's face and having droplets land on one's face.
This made me wonder 'Can coronavirus spread through open eyes?' (https://www.quora.com/Can-coronavirus-spread-through-open-eyes) given I had heard it was spreading through the lungs, but I'm not actually sure about the eyes.
Track your sleep quality and make sure you are getting enough. There are smartphone apps (like Sleep Cycle) that can do this. Your immune system is one of the first things to go with even mild sleep deprivation, which makes you more susceptible to infection. You may have to adjust the timing or dose of your caffeine intake. You might also consider melatonin (see Scott Alexander's guide for optimal timing and dose).
Gargling (even with water) might be a relatively good intervention: https://pubmed.ncbi.nlm.nih.gov/16242593/
Gargling with salt water is a traditional method of treating sore throat/tonsillitis/swollen sub-mandibular lymph nodes.
I'm getting a little obsessed with garlic so I'd gargle with a garlic solution after the salt...
Here's a guesstimate model I made to try and figure out when hospitals will become overwhelmed. Lots of model uncertainty here that I'd appreciate advice on, but the current prediction is that there will be a hospital bed for you if you get infected in the bay area within the next 6 days (95% confidence within the model: actual confidence is much lower).
I'm super happy to see quantitative models, but moving this to comments because it doesn't cash out into specific advice.
There's a theory that BCG vaccine (TB) helps strengthen you against corona, I'd recommend getting it if you haven't, or especially for your older relatives (given that the cost/side effects is well-understood and near-zero, whereas the benefits based on the below could be serious):
https://www.mpg.de/14610776/immune-boost-corona-virus https://www.sciencemag.org/news/2020/03/can-century-old-tb-vaccine-steel-immune-system-against-new-coronavirus
https://foreignpolicy.com/2020/03/24/coronavirus-vaccine-health-care-workers-bcg/
https://www.france24.com/en/20200326-australians-trial-tb-vaccine-to-fight-coronavirus
https://www.medrxiv.org/content/10.1101/2020.03.24.20042937v1 (looking at the correlation between vaccination rates by country and corona spread).
Very speculative: there are different strains of BCG, and allegedly the old (Soviet/Japan/Brazil) type/types is better. This could theoretically explain the different corona case loads between West/East Germany and between Japan + Thailand + Taiwan vs China + Iran (different vaccine strains).
Here are images showing differing corona case loads between East/West Germany (East uses/used the Soviet vaccine), supposedly the population density does not explain this (though note travel patterns, testing rates, etc. are probably all different):
Much more at https://www.jsatonotes.com/2020/03/if-i-were-north-americaneuropeanaustral.html?fbclid=IwAR2MKAgIt2IRjPSf_S9F4HozW4z7BWjH9_9D5p3RmGGJtdh2wp5gkpdzOj8&m=1. If someone who actually understands vaccines could read this and provide thoughts and vet, that'd be great. If it does end up making sense, please do spread, given the high expected value benefit here. I just don't know how easy it'd be to find old (Soviet etc.) style vaccines in the West.
I'd recommend getting it if you haven't, or especially for your older relatives (given that the cost/side effects is well-understood and near-zero, whereas the benefits based on the below could be serious):
I would recommend doing more research before making recommendations like the above. tb-throwaway.
Start here: NHS Who should have BCG?.
To quote one line that you could investigate:
There's no evidence the BCG vaccine works for people over the age of 35.
If hospitals are overwhelmed, it's valuable to have a component of the hospital treatment plan for pneumonia on-hand to treat either yourself or others who have it especially bad. One of these is oxygen concentrators, which are not sold out yet and are ~$400 on Amazon. This doesn't deal with especially severe cases, but for cases which fall in the "shortness of breath, low blood oxygen" class without further medical complications, it'd probably be useful if you can't or don't want to go to a hospital due to overload. https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected mentions oxygen treatment as the first thing to do for low blood oxygen levels.
I think I would feel guilty if I bought one of those, and then learned later that they're sold out, and the people building temporary hospitals can't get them.
Good idea. I purchased an oxygen concentrator. However, you might wish to use the device on a low pressure setting (or use it in "pulse" mode instead of "continuous" mode) because I'm hearing some rumors that oxygen therapy can be counterproductive:
...Professor Liu Liang also said that if the mucus components are not resolved in the treatment, the use of oxygen alone may not achieve the purpose of treatment, and sometimes even counter-productive, pushing the mucus deeper and wider, aggravating the patient's hypoxia.
WHO report indicated that 75% of severe cases only needed oxygen. Only 25% needed forced respiration + suction. So this seems good.
Do your shopping in bulk in order to minimize the time you spend public. Or do your shopping online and have it delivered.
The more time you spend in public, the higher the risk you get infected. Shopping in bulk minimizes the time you spend in public, and thus lowers the risk that you get infected. For example, stocking up at Sam's Club versus going to the supermarket twice a week.
I suspect that for most people, the downside of shopping in bulk or shopping online is going to be very minimal. In many cases I suspect that it is optimal even without the coronavirus being a thing.
Also consider the experimental benefit. If you don't have much experience with shopping in bulk or online, trying it out for a few weeks will give you a better sense of what your true preferences are.
Advice: now may be a good time to learn to meditate. Deaths from coronavirus are due mostly to breathing problems from pneumonia, which is the main explanation for why older people are more likely to die. There is evidence that meditation is good for pneumonia specifically http://www.annfammed.org/content/10/4/337.full and lowers oxygen consumption generally https://journals.sagepub.com/doi/full/10.1177/2156587213492770. I didn't read the studies carefully to see how trustworthy they are, but this conforms well with my understanding and limited experience of meditation. Meditation is also known to be good for mitigating stress, which will obviously be beneficial in the coming months.
This is likely to: (a) last for months, not weeks - so don’t bother stockpiling, you can’t store enough to outlast it. (b) affect 60-80% of an unimmunised population (all of us) with a doubling time in confirmed cases of 2-3 days initially. (c) produce minimal symptoms in the majority of cases (by minimal I mean nothing you cannot handle with over the counter analgesics, plenty of rest and your favourite hot drinks) just like the currently endemic corona viruses. (d) be moderately lethal for older people, especially smokers & those with existing respiratory / cardiovascular conditions. (e) become endemic (annual, like flu & colds) unless we get a vaccine.
Solution? Keep calm & carry on, hoping your government is transparent and has your best interests at heart.
If it's more important for you to avoid contracting the virus right now than it is for others, schedule any doctor's appointments you are going to for first thing in the morning. Reasoning: seems like hospital contamination should rise throughout the day as more and more people pass through and then drop during nightly cleanings. Similarly for any needed outings, do it in the morning, because though the virus can survive for days on surfaces, presumably it's safer to touch just after an 8 hour break from people than just after a 2 minute break from people. No idea of effect size but I don't see why these mechanisms would be wrong.
Get fully vaccinated, preferably using the Moderna vaccine.
https://www.microcovid.org/paper/14-research-sources#moderna--pfizer says "[the] CDC released a study showing 90% reduction in all cases (symptomatic + asymptomatic) 14+ days after participants received Moderna or Pfizer’s vaccine".
It makes sense for anyone competent enough to give consent for the vaccination unless you are known to have an allergic reaction to a component of all available vaccines.
While I suspect the option for non-cash payment will remain it is possible that in some cases having cash on hand might be needed. If so, you probably don't want to go to the bank/ATM and get something that may have passed though a bunch unknown hands.
I am thinking that suggests two things.
1) Make an assessment of your potential cash needs and get them sooner rather than later. Two reasons here. Lowers the chances of being contaminated. You can then set it aside as well as do some sterilization and let sit (to dry?).
2) You might not want to get large bills but more smaller denomination. That way you can simply leave the change and not worry about accepting anything back.
Again, might have been suggested but a quick search on cash and currency didn't get any hit.
Advice: drink a mouthful of water every 15 minutes. This is speculative (facebook post from a friend of a friend). The rationale is that if you have virus particles in your mouth, rinsing them into your stomach (where the stomach acid kills them) will prevent them from getting into your respiratory system. [edit: retracted, seems to be downstream from a fake news article. Drinking water is still good, but looks like this pathway is not realistic]
Most advice here seems to be of the form "here's a thing that has a benefit" or "here's a thing that has a benefit, and the cost is low". But without an estimate of the relative magnitudes of the costs and benefits, it's hard to know whether taking the advice is worth it. I wish that more advice included this type of cost-benefit analysis, perhaps with a parameter of how bad things are so that one could say, for example, "it's worth it to do this thing if you think X proportion of your city will eventually be infected".
There is probably an optimal humidity level, but looking at data from other viruses is producing very mixed results about what that level might be. Does anyone else want to dig through some more papers? This might also be a case where better data will be available in a few weeks.
This study found that environmental humidity was positively correlated with nCoV rate of spread. This paper measured surface persistence of SARS, and found that it persisted less at moderate relative humidity (50%) than at low (20%) or high (80%) humidity. This paper tested MERS-CoV, and found that increasing humidity from 40% to 80% decreased persistence on steel, but increased persistence on plastic.
How much do I need to worry about reinfecting myself? If I catch COVID-19 and enter perfect quarantine, does leaving viral particles on the lightswitch and picking them up the next day matter?
So the SARS virus exhibits, at least in the lab, Antibody Dependent Enhancement which is what can allow a virus to affect you multiple times. Here's a paper on it. Since COVID-19 is related to SARS it seems plausible the reports of reinfection are real. I don't understand this enough to say much more about it.
Is this a good place to put questions that I want answered?
Is there some reliable source on the triggers for quarantining one's self? Both immediate triggers (when x happens, I will not leave the house again until y happens), and warning signs (when z happens, I'm going to leave the city, in preparation for quarantine).
I've been struggling with the question of whether I should leave the SF area to go to my parent''s house in the suburbs of Virginia, and I expect other people are facing similar conundrums. I'll share my thoughts on it below and would welcome any advice especially anything that I have not considered.
Background: My parents (both 50 - 60) live in a detached house in the Virginia suburbs. It's very large with 3 floors and many bedrooms and has an inlaw unit. I currently live with 3 roommates, one of whom is my partner, in a tiny apartment in downtown San Francisco. 2 of those roommates have jobs in SF, another is unemployed but unconcerned with the virus, and I'm unemployed, living off saved income and very concerned. Currently we are all asymptomatic, but my partner did fly to Canada last week and has been isolating with no symptoms.
I'm considering whether to take my partner and fly to Virginia to be in our parent's house, likely early next week. Thoughts
The killer advice here was masks, which was genuinely controversial in the larger world at the time. When we wrote a summary of the best advice. two weeks later, masks were listed under "well duh but also there's a shortage".
Of the advice that we felt was valuable enough to include in the best-of summary, but hadn't gone to fixation yet, there were 4.5 tips. Here's my review of those
Cover your high-touch surfaces with copper tape
I think the science behind this was solid, but turned out to be mostly irrelevant for covid-19 because it was so dominantly airborne. The tape turned out to be hard to remove, which caused a bunch of annoyance for people who moved a few months later.
Treat newly delivered packages as contagious for 48 hours.
Also made irrelevant by the low fomite rate
Take vitamin D supplements daily
The evidence for this has only gotten stronger since we wrote this up, although vitamin D has such a strong fandom you can never be sure.
Buy electrolytes to drink if you get ill
I don't know anyone this ended up being a big deal for, but it was low cost and I still believe there are low-frequency scenarios where it would have been very helpful.
Maybe: Buy a pulse ox...
For food, I just purchased a week's worth of Soylent powder. Here was my reasoning (feel free to critique because I might purchase more):
I'm wondering how well viruses stick to/survive on clothing. In trying to avoid touching my face, I've occasionally resorted to using sleeves of my hoodie instead – which I also use to touch surfaces like door knobs or light switches. Should I use the elbow for those instead?
A question (using the comment feature because I do not yet know what "ask related question" actually does): Is it advisable to use reusable (rather than disposable) filter masks, if available? (They are obviously much more expensive, but they also have much higher availability right now in many cases; and people who attend Burning Man, or have hobbies involving noxious fumes, may already have them.)
If so, what are the right precautions to take? Obviously throwing away a disposable mask eliminates all possibility that it will later create a contamination ha
...Learn to wash you hands well - then do so several times a day, and use alcohol based hand sanitizer in-between.
Here's a video explaining how to do it: https://www.youtube.com/watch?v=eZw4Ga3jg3E&feature=youtu.be&t=64
Note: In order for this to work well, keep your nails short, and don't wear rings.
Related question: at what point should university students begin partial-quarantine measures such as not going to large classes and not going to cafeterias?
I'm concerned about the cafeteria things especially, because it seems like a pretty potent vector for transmission and also relatively avoidable by just buying/preparing your own food. At the minimum, I suspect that doing things like bringing your own utensils/plates that you've disinfected to be a reasonable precaution, although all the food is sort of sitting out so I'm not sure if that's even a thing
...While working at home while doing laboratory research is not doable, my hours are flexible and I am able to shift my workload between writing/theory work and wet-lab work. So, I am in the process of closing down several of my ongoing time-intensive wet-lab experiments, shifting my daytime to writing up existing research in my apartment, and moving my labwork to be more nocturnal when fewer people are around and I am not tempted by open eateries on the campus I work at. As one of the globetrotting academic class I am way fewer degrees of separation from so many places on Earth...
Similar things could be relevant to those fortunate enough to have flexible work arrangements.
[This should have been posted under answers. Mods, please move this if you can.]
Buy Chloroquine or Hydroxychloroquine: https://www.jstage.jst.go.jp/article/bst/advpub/0/advpub_2020.01047/_article
Reputable online pharmacies:
(I used the first one but the order
...Hmm, Wikipedia tells me that Choloquine mildly suppresses the immune system, and also that it has a low theraputic index -- that is, the ratio between an effective dose and an overdose is relatively small -- and that it is "very dangerous in overdose". This does not sound like a drug that is necessarily very safe to self-administer, or recommend to people to do that, without substantial research.
EDIT: Additionally, the article you link has very little information in it. It lists a bunch of clinical trials but I can't figure out whether it's possible for me to see the results. It's not an academic paper in any real sense, just some kind of summary of other results. The only citation for the "multicenter clinical trials" given is to a press briefing by the Chinese government. There is one relevant citation to an article in Nature, but it is short and contains limited information, and is listed as a "Letter to the Editor" presumably meaning it's a preliminary result not subject to peer review.
None of this inherently means the science isn't good, but I think the risks of suggesting that people consider self-medicating with an apparently-dangerous drug are not justified by the flimsy evidence so far available.
Sorry, I wrote that in a hurry and didn't have time to report all of my reasoning. According to Wikipedia:
Hydroxychloroquine was approved for medical use in the United States in 1955.[1] It is on the World Health Organization's List of Essential Medicines, the safest and most effective medicines needed in a health system.
Yes the therapeutic index is low and I'm not a doctor but I don't think that mean it's easy to overdose if you follow direction. Otherwise it wouldn't be a very widely prescribed drug (in parts of the world where malaria is common). I haven't seen any reports or warnings of people overdosing after following recommended dosages (ETA: except after taking it for years). I only found accidents or suicides.
And you're right the paper is not a normal academic paper, but that is understandable given the fast moving circumstances. I do think it's pretty strong Bayesian evidence that Chloroquine and Hydroxychloroquine do more good than harm. Suppressing the immune system may be part of how it works (i.e., the immune system can do a lot of damage to one's lungs in the course of fighting infection).
Hi! I'm from China-yes, exactly the place where COVID-19 was born and ruined our Spring Festival completely. After months-long battle with the virus, now the confirmed case of COVID-19 has down to an alltime low. But it saddens me to see that this virus seem to spread across other countries,South Korea,Japan,Iran,Italy etc. Here I'd like to share with you some advice that Chinese goverment used to prevent the virus from infecting more people.
1.Intially, the government advised people to stay at home. But soon,the advice escalated to ne...
What makes you think this advice is good, or have the sources provided their own justification? This thread is specifically for justified advice, not high-prestige advice.
I think everyone should be stocking up on at least a month of food because survival-grade food is cheap and has at least a10% chance of being very useful to you at some point, either in this pandemic or for a different emergency.
As this answer mentions, copper tape kills diseases. And most of the spread seems to come from hand-to-surface-to-face. With those thoughts, I'm wondering if there is some sort of glove you could wear that makes spread less likely.
(Meta: unsure if it's ok to post an on-topic RFC here. Apologies in advance)
Should I sign up for cryonics ASAP?
Background: 23 y/o male in NYC. No known pre-existing health conditions. Mild -> moderate interest in cryonics; in a world without ncov, etc. would probably have a 30-60% chance of signing up.
Should I expect a faster infection rate on my country (Brazil) because most people here use paper money to make trades? Should I recommend people to stop using paper money and instead opt for a contactless card? Most people don't have access to banking services; so is there any option for them?
Advice: when prepared food contamination risk becomes high, order in food that can be heated and microwave it thoroughly before eating
Wear gloves when in public places.
Washing your hands for 10-20 seconds properly as recommended is hard, as is not touching your eyes, mouth, face.
This becomes easier when wearing gloves.
I suspect that the rate of spread is <1 in firstworld countries. I predict that we will see a few people who have travelled abroad catch the virus. If the virus does start spreading out of control, there will be time to stock up when the numbers are in the thousands. (In the UK) I would be more worried if I was in china or south korea.
Edit: I no longer believe this
Monitor the situation, e.g., with dashboards like this: https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
{kind=link}
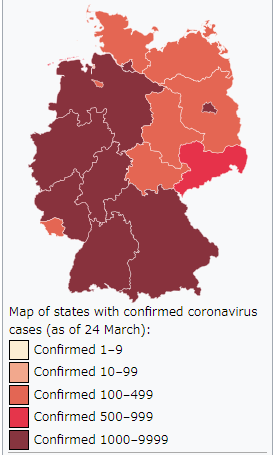{kind=link}
(Added: To see the best advice in this thread, read this summary.)
This is a thread for practical advice for preparing for the coronavirus in places where it might substantially grow.
We'd like this thread to be a source of advice that attempts to explain itself. This is not a thread to drop links to recommendations that don’t explain why the advice is accurate or useful. That’s not to say that explanation-less advice isn’t useful, but this isn't the place for it.
Please include in your answers some advice and an explanation of the advice, an explicit model under which it makes sense. We will move answers to the comments if they don't explain their recommendations clearly. (Added: We have moved at least 4 comments so far.)
The more concrete the explanation the better. Speculation is fine, uncertain models are fine; sources, explicit models and numbers for variables that other people can play with based on their own beliefs are excellent.
Here are some examples of things that we'd like to see:
One piece of information that has been lacking in most advice we’ve seen is when to take a particular action. Sure, I can stock up on food ahead of time, but not going to work may be costly– what’s your model for the costs of going so I can decide when the costs outweigh the benefits for me? This is especially true for advice that has inherent trade-offs– total quarantine means eating your food stockpiles that you hopefully have, which means not having them later.